



There is perhaps no framework in modern sports medicine that has spread faster, or generated more debate, than Relative Energy Deficiency in Sport (REDs).
For some clinicians, REDs has become an essential lens through which to understand underperformance, menstrual dysfunction, fatigue, recurrent injury, impaired recovery, and long-term health consequences in athletes and dancers. For others, the framework has expanded so broadly that it risks becoming clinically nonspecific: a model capable of explaining almost everything, and therefore potentially difficult to falsify.
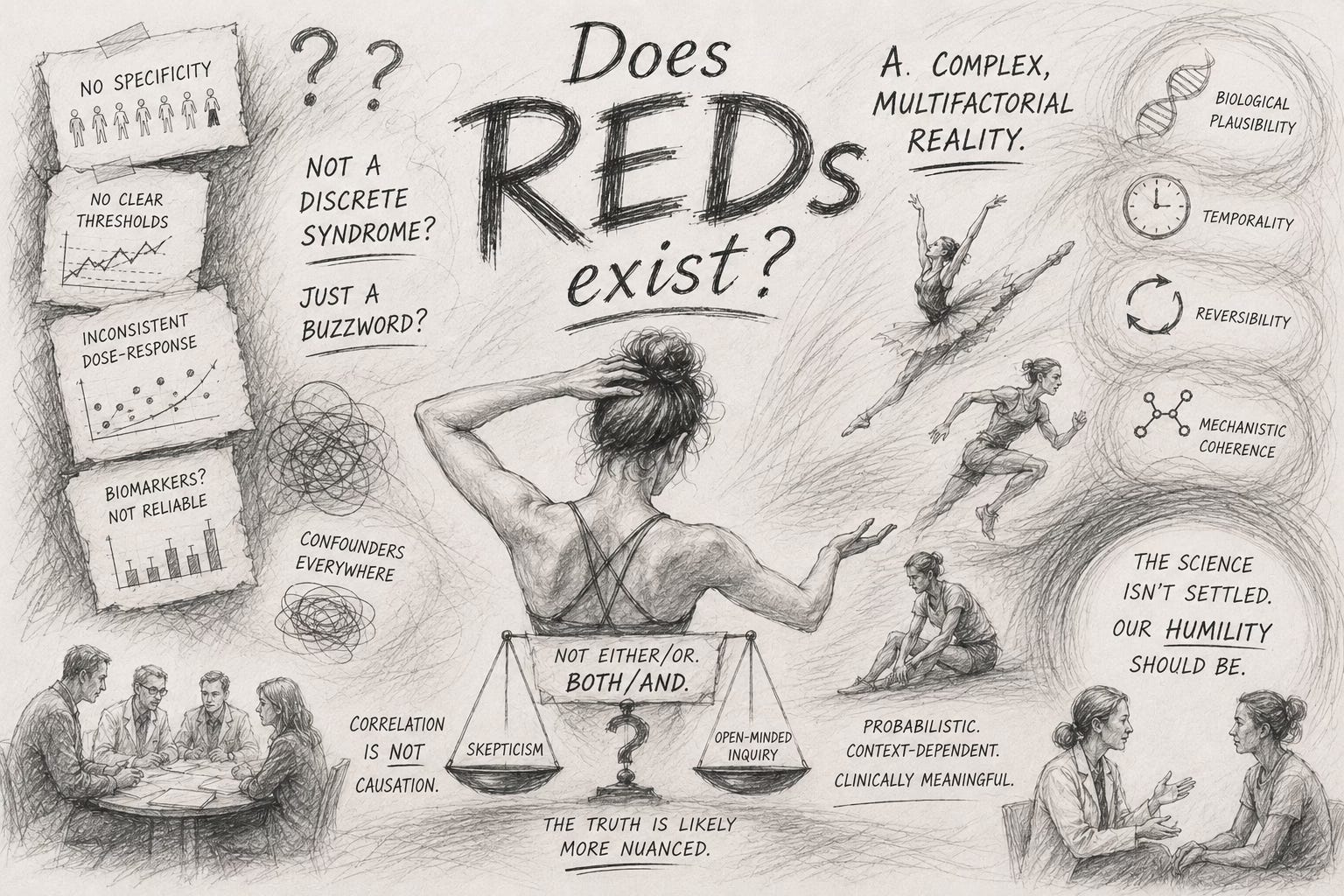
So the question asked by a group of scientists - ‘Does REDs exist?- sounds deceptively simple. And at first glance, it appears to be a scientific question.
In practice though, it may be a philosophical, clinical, and systems-level question instead.
Because the dispute is not merely about whether low energy availability can impair human physiology. Few serious clinicians dispute that it can. The deeper disagreement concerns causality, specificity, evidence, and how medicine should reason under uncertainty.
And perhaps most importantly: what happens when simplified physiological models meet complex human beings.
How We Got Here
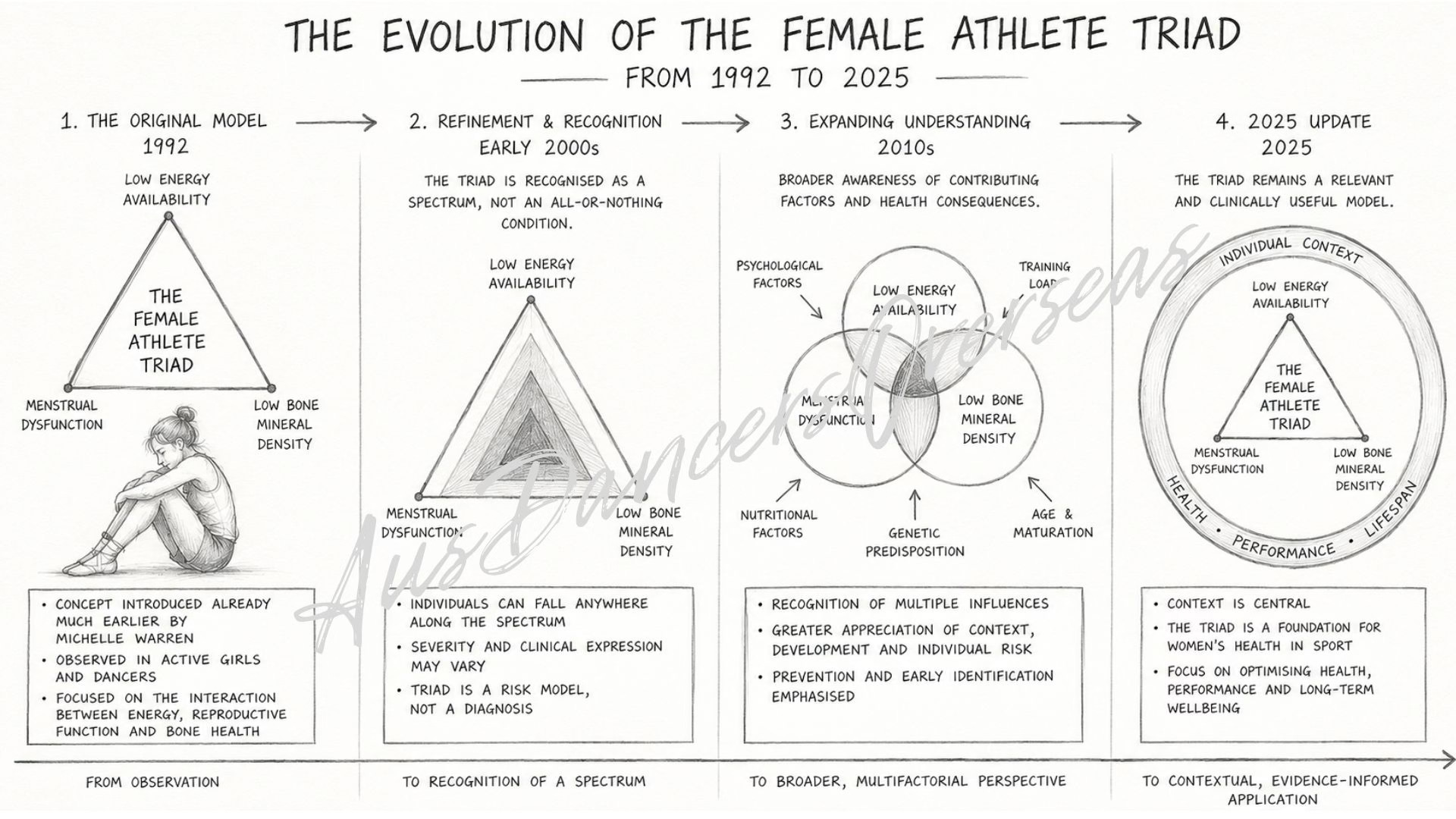
The roots of this discussion predate REDs by decades. The original Female Athlete Triad framework emerged from observations that many active women experiencing menstrual dysfunction also exhibited impaired bone health and inadequate energy intake. Importantly, some of the earliest observations came from ballet populations. Michelle Warren’s 1980 publication on pubertal progression and reproductive function in girls described delayed maturation and menstrual disturbances in young dancers exposed to intensive training environments.
MICHELLE WARREN’S PUBLICATION
The Triad was conceptually elegant because it was relatively constrained:
low energy availability
menstrual dysfunction
impaired bone health.
The relationships were biologically plausible, clinically observable, and comparatively measurable. Over time, the model evolved from a strict ‘three-part syndrome’ into a spectrum-based framework acknowledging varying degrees of physiological adaptation and severity.
Yet even in its refined form, the Triad remained relatively focused. And that focus has always been one of its strengths.
The Expansion from Triad to REDs
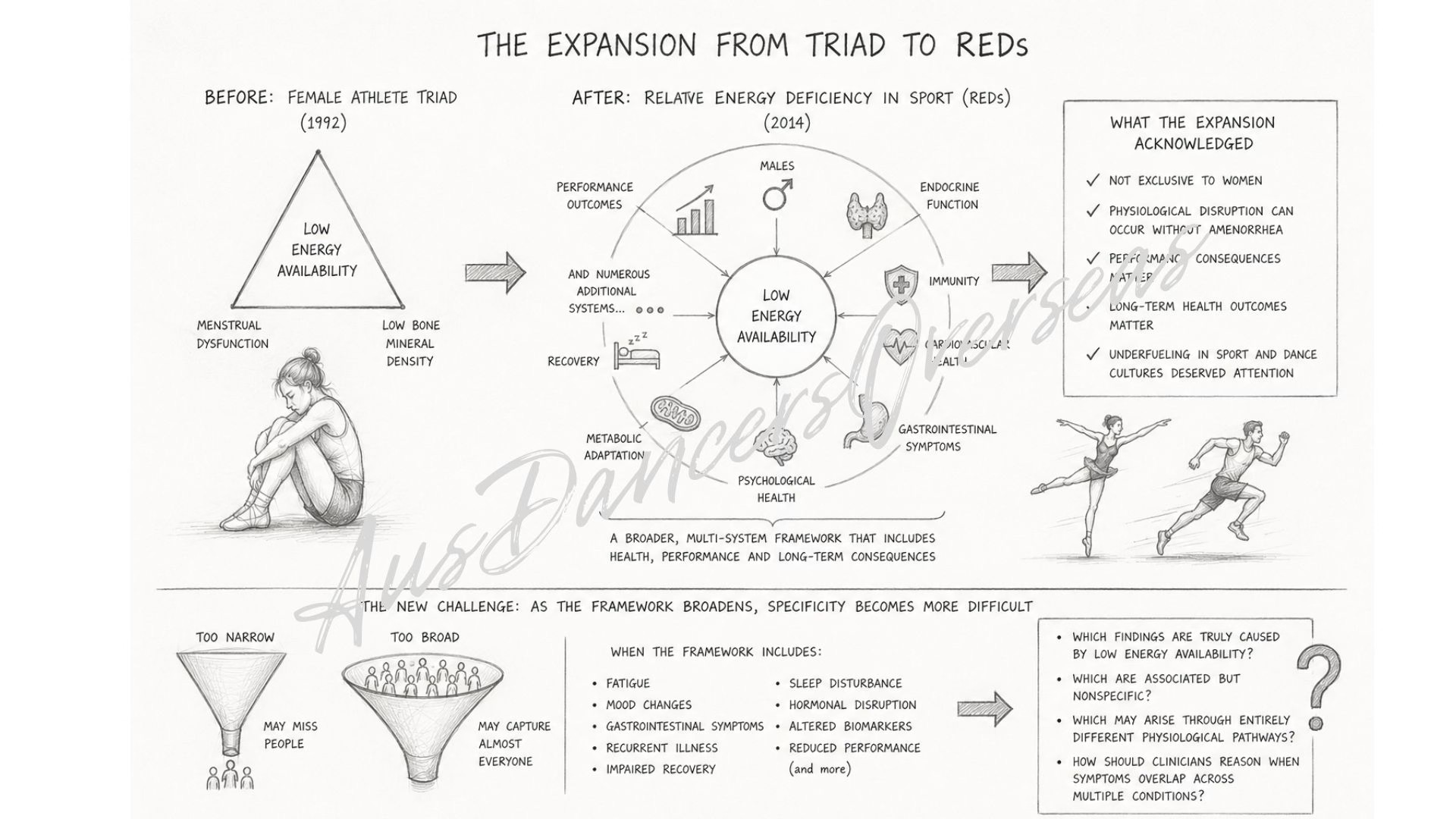
In 2014, the International Olympic Committee introduced Relative Energy Deficiency in Sport (REDs), substantially broadening the framework. The model expanded beyond female athletes and reproductive health to include:
males
performance outcomes
endocrine function
immunity
cardiovascular health
gastrointestinal symptoms
psychological health
metabolic adaptation
recovery
and numerous additional physiological systems.
The expansion was clinically meaningful in many ways.
It acknowledged that low energy availability is not exclusive to women. It highlighted that athletes may experience significant physiological disruption even in the absence of amenorrhea. It emphasized performance consequences alongside long-term health outcomes. It also brought overdue attention to underfueling within sport and dance cultures where chronic restriction had often been normalized.
In many respects, REDs increased awareness where awareness was desperately needed. But the expansion also introduced a new challenge:
The broader a framework becomes, the more difficult specificity becomes.
A narrow model may miss people. A broad model may begin to capture almost everyone. And once a framework includes fatigue, mood changes, gastrointestinal symptoms, recurrent illness, impaired recovery, sleep disturbance, hormonal disruption, altered biomarkers, and reduced performance, questions inevitably emerge:
Which findings are truly caused by low energy availability?
Which are associated but nonspecific?
Which may arise through entirely different physiological pathways?
And how should clinicians reason when symptoms overlap across multiple conditions?
Overtraining and the Seduction of Linear Models
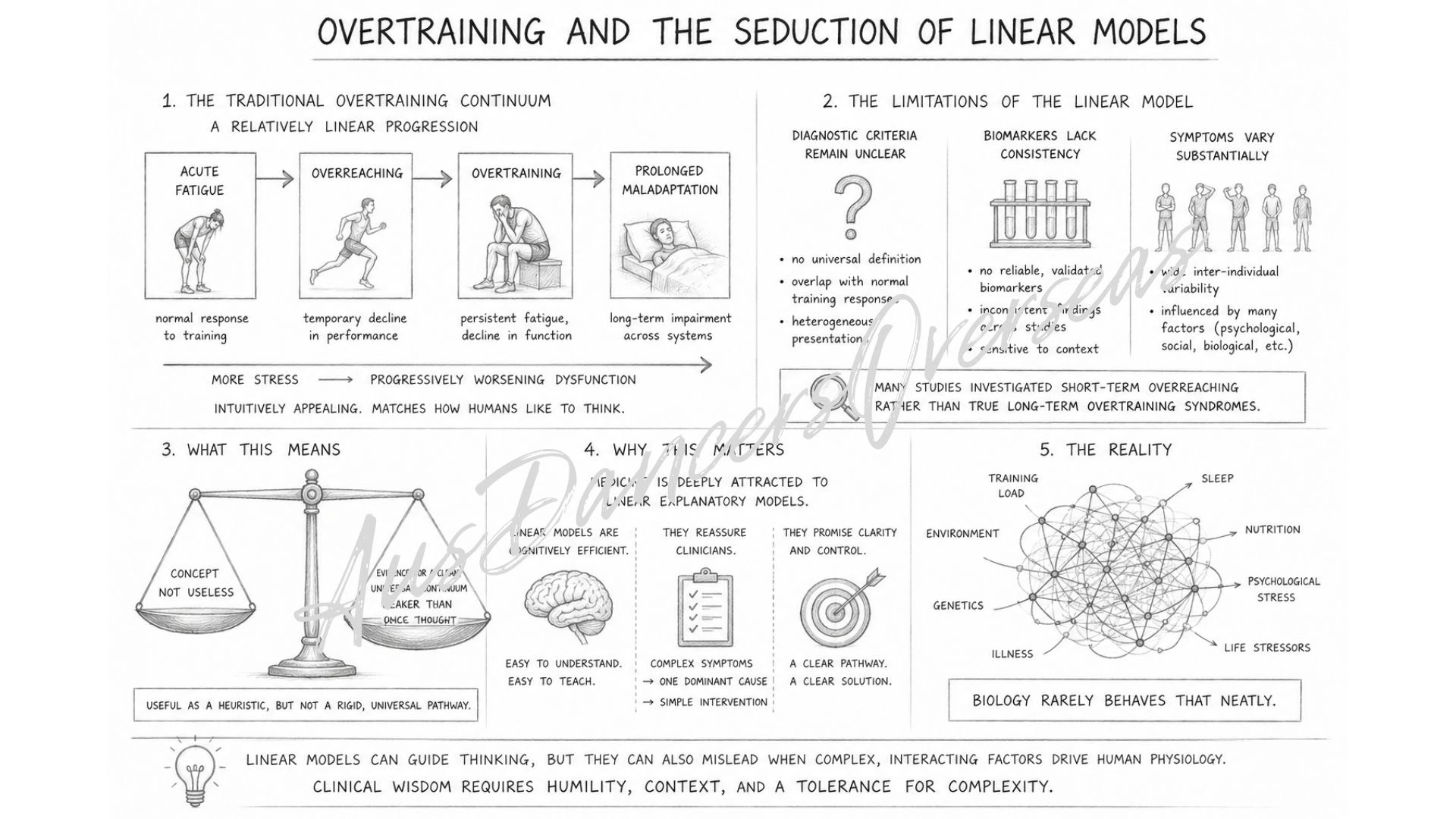
Long before REDs, sports medicine had already encountered a similar problem through the concept of overtraining syndrome. The traditional overtraining continuum proposed a relatively linear progression:
acute fatigue → overreaching → overtraining → prolonged maladaptation.
The model was intuitively appealing. It matched the way humans like to think:
more stress leads to progressively worsening dysfunction.
Yet over time, researchers began acknowledging significant limitations: diagnostic criteria remained unclear, biomarkers lacked consistency, and symptoms varied substantially between individuals.
Additionally, many studies investigated short-term overreaching rather than true long-term overtraining syndromes.
The concept itself was not necessarily useless. But the evidence supporting a clean, universal continuum proved weaker than many had assumed. This matters because medicine is deeply attracted to linear explanatory models. Linear models are cognitively efficient; they reassure clinicians that complex symptoms can be traced back to a single dominant mechanism.
But biology rarely behaves that neatly.
The REDs Critique
In 2024, Asker Jeukendrup and colleagues published a provocative paper asking directly:
‘Does Relative Energy Deficiency in Sport (REDs) Syndrome Exist?’
The paper did not argue that low energy availability is harmless, nor did it deny that athletes can become physiologically compromised by insufficient fueling.
Instead, the critique centered on something more specific: whether the evidence currently justifies attributing the vast constellation of REDs-associated symptoms primarily to low energy availability itself.
The authors raised several concerns:
many REDs symptoms are highly nonspecific
causality is difficult to establish
diagnostic thresholds remain unclear
confounding variables are substantial
and the framework risks becoming difficult to falsify.
Some clinicians experienced this critique as dismissive or even dangerous, particularly those working daily with severely underfueled athletes and dancers whose recovery clearly improves with nutritional rehabilitation. So that reaction is understandable, for many practitioners do observe obvious clinical consequences of chronic underfueling.
But the existence of clear cases does not automatically validate every proposed causal pathway within a broad framework. And this is where the debate often becomes polarized in unhelpful ways.
The Problem with Binary Thinking
The current discourse sometimes collapses into two simplistic positions:
‘REDs explains everything’.
versus
‘REDs does not exist’.
Neither position adequately reflects clinical reality. The challenge is not that low energy availability never contributes to dysfunction.
The challenge is that human physiology is rarely monocausal.
Consider symptoms commonly discussed within REDs frameworks:
fatigue
orthostatic intolerance
gastrointestinal disturbance
mood changes
sleep disruption
recurrent injuries
altered lipid profiles
menstrual disturbances
impaired recovery.
These symptoms can indeed emerge in the context of chronic underfueling.
But they may also emerge through numerous overlapping mechanisms:
neurodivergence
hypermobility syndromes
autonomic dysfunction
chronic stress
inflammatory disease
trauma-related physiological adaptation
endocrine disorders
infection
gastrointestinal pathology
inadequate sleep
psychological strain
or combinations of all of the above.
In dance medicine particularly, this overlap becomes clinically important: a hypermobile or neurodivergent dancer may present with fatigue, gastrointestinal symptoms, anxiety, orthostatic intolerance, altered lipid markers, recurrent injury, and autonomic dysregulation long before severe low energy availability enters the picture.
If clinicians prematurely collapse all symptoms into a REDs framework, important contributors may be overlooked.
Yet the opposite risk also exists: assuming symptoms are ‘just stress’, ‘just anxiety’, or ‘normal for dancers’ when chronic underfueling is genuinely driving physiological compromise.
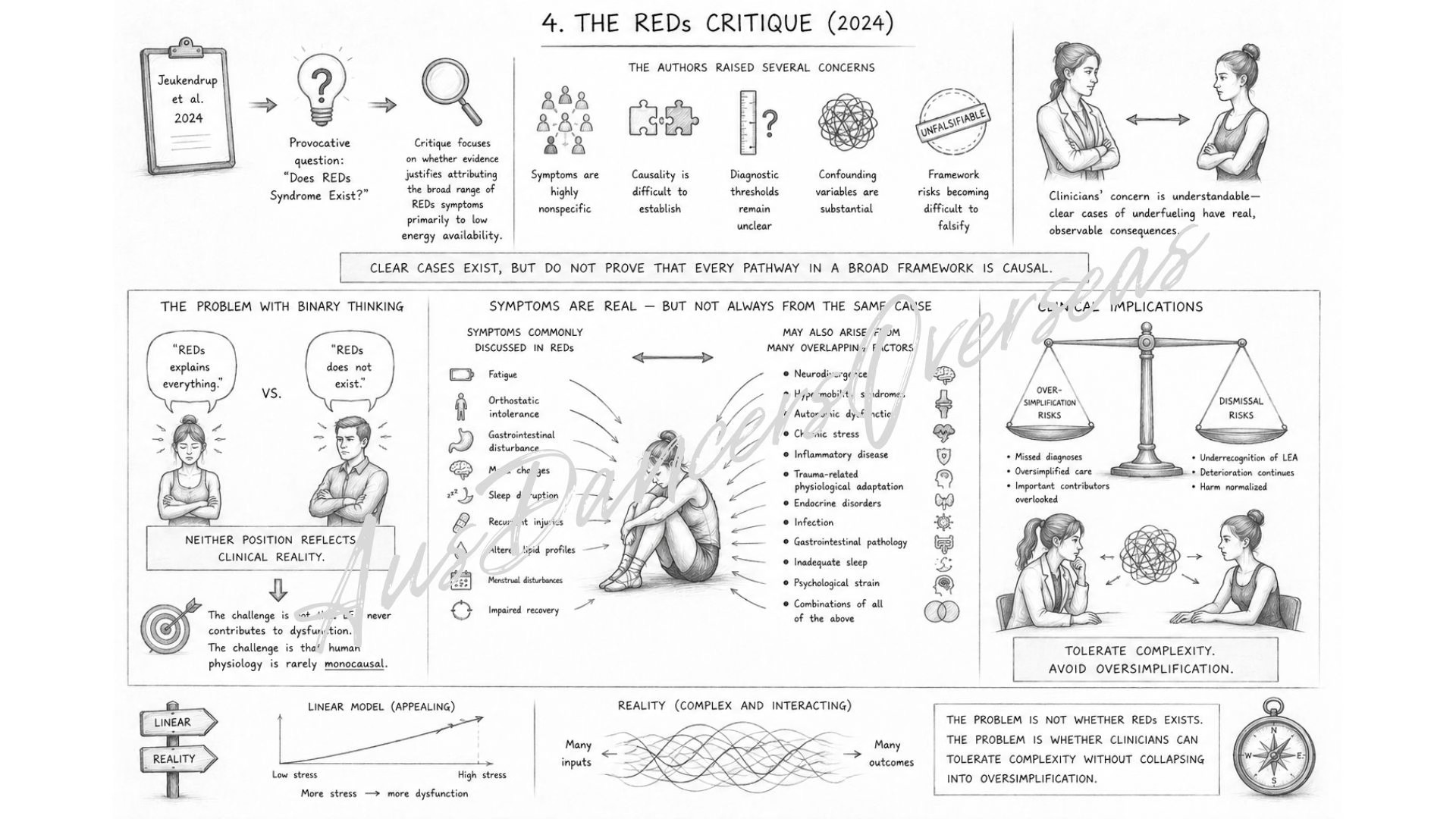
The problem, therefore, is not whether REDs exists. The problem is whether clinicians can tolerate complexity without collapsing into oversimplification.
Enter Allostatic Load
Perhaps the most useful development in this discussion is the increasing interest in allostatic load and systems-based models of physiological stress.
Allostasis refers to the body’s ability to maintain stability
through adaptation when exposed to stress.
Allostatic load describes the cumulative physiological burden imposed by repeated or chronic stress exposure across multiple systems. Importantly, this framework does not prioritize a single stressor and recognizes interacting physiological demands instead:
training load
psychological stress
inadequate sleep
social threat
trauma
illness
nutritional insufficiency
neurodivergence
environmental instability
chronic inflammation
autonomic strain.
Under this lens, low energy availability remains highly relevant - but as one component within a broader adaptive network rather than necessarily the sole initiating cause. This perspective may better reflect what clinicians actually encounter in practice: not isolated syndromes, but overlapping systems under cumulative strain.
A dancer navigating perfectionism, restrictive eating, chronic sleep disruption, psychological pressure, gastrointestinal disease, and intense training load may not fit neatly into a single diagnostic framework. Yet the physiological burden is still real, and clinically consequential.
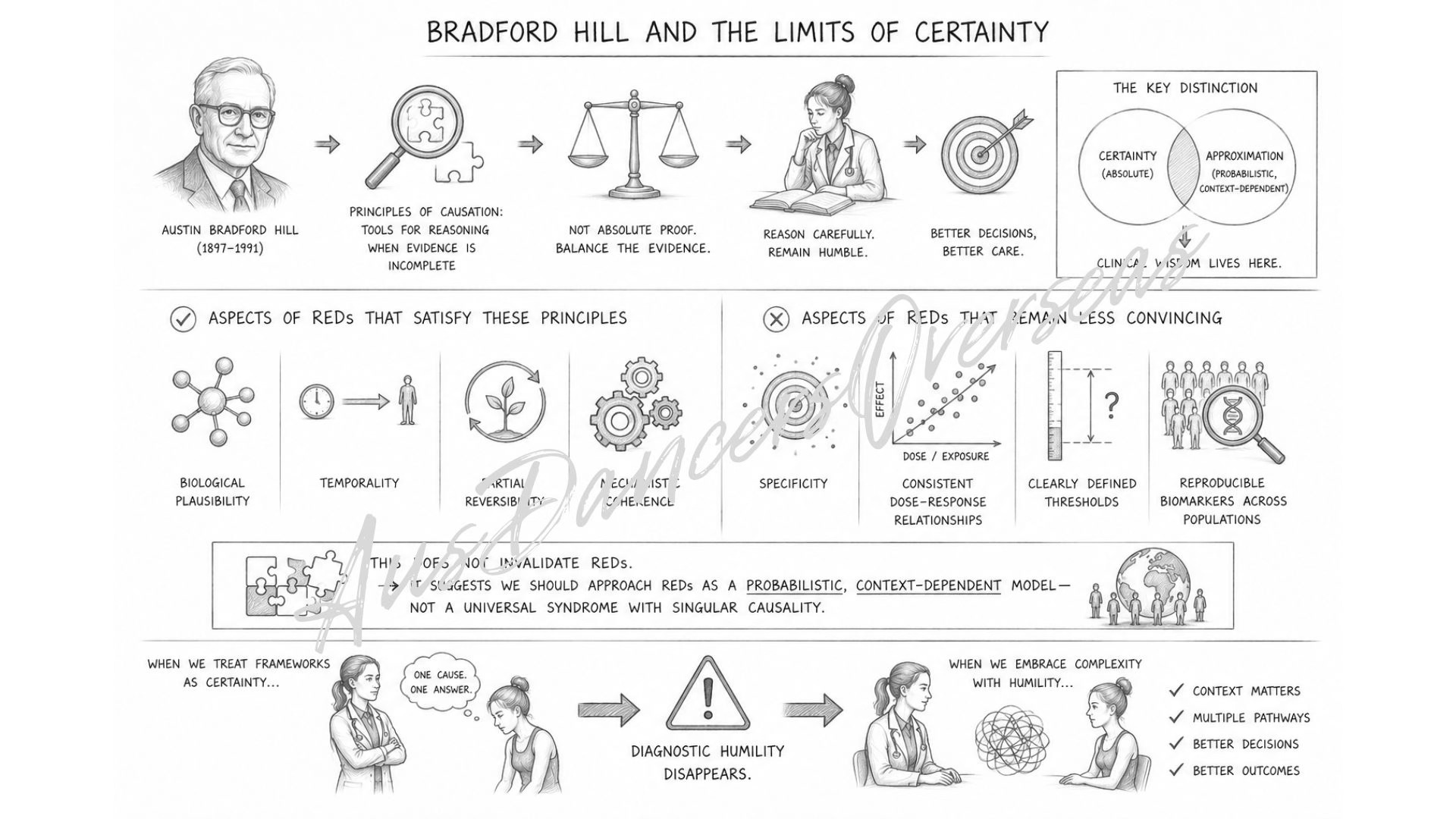
Bradford Hill and the Limits of Certainty
One reason the REDs debate remains unresolved is that causality in medicine is rarely absolute: Austin Bradford Hill’s principles of causation were never intended to produce perfect certainty. They were designed to help clinicians reason carefully in situations where evidence remains incomplete.
Some aspects of REDs satisfy these principles reasonably well:
biological plausibility
temporality
partial reversibility
mechanistic coherence.
Others remain less convincing:
specificity
consistent dose-response relationships
clearly defined thresholds
reproducible biomarkers across populations.
This does not necessarily invalidate the framework, but it does suggest that clinicians should approach REDs as a probabilistic and context-dependent model rather than a universally discrete syndrome with singular causality. That distinction matters profoundly. Because once clinicians begin treating frameworks as certainty rather than approximation, diagnostic humility disappears.
The Real Clinical Risk
The greatest danger is not whether REDs ‘exists’.
The greatest danger is getting the reasoning wrong.
If every symptom is interpreted through a REDs-lens:
important diagnoses may be missed
complex physiology may be oversimplified
patients may become reduced to energy balance equations.
But if clinicians dismiss REDs entirely:
genuine underfueling may go untreated
athletes may continue deteriorating
severe physiological consequences may be normalized or minimized.
Medicine rarely offers perfect diagnostic clarity. And healthcare professionals working with dancers and athletes are often forced to make decisions using incomplete, evolving, and imperfect evidence. A reality that is uncomfortable, but unavoidable.
Perhaps this is why the REDs debate continues to recur. It is not merely a dispute about one syndrome. It reflects a much broader tension within medicine itself:
the tension between simplified models and complex humans.
As Siddhartha Mukherjee wrote in The Laws of Medicine:
‘Medicine is not the pursuit of perfect certainty,
but the practice of reasoning carefully in its absence.’
That may ultimately be the most clinically useful conclusion of all.
Thanks for reading. Until next time …
